In the social interactions of our daily lives, the frontalis muscular tissue plays a significant role. Given that it is the only muscle that elevates eyebrows, its feature exceeds simply maintaining them out of one’s visual field; it is also essential for sharing feelings and nonverbal communication. The frontalis muscle is antagonistic to the procerus muscle mass, the corrugator supercilii muscle, and the orbicularis oculi muscle mass.
The frontalis, corrugator, procerus, and orbicularis muscles all have cutaneous insertions and assemblage at the glabella. The orbital edge, where their respective motions and pressures can lead to cutaneous rhytids (frown lines, smile lines, forehead lines, horizontal nasal lines)—the balance between these muscles figures out the position and form of the brows.
What is the Frontalis Muscle mass?
How well is your frontalis muscle mass functioning? The majority of individuals have no idea what the frontalis muscle is or where it lies. It lies on top of your forehead.
You can examine the performance of your frontalis muscular tissue by adhering to these simple steps:
- Look for a mirror
- Stand in front of the mirror and also look at your representation
- with elevated eyebrows
- When you explored the mirror while raising your brows, did your temple come wrinkled? After that, your frontalis muscle mass seems to be working fine.
Frontalis Muscular Tissue: Definition
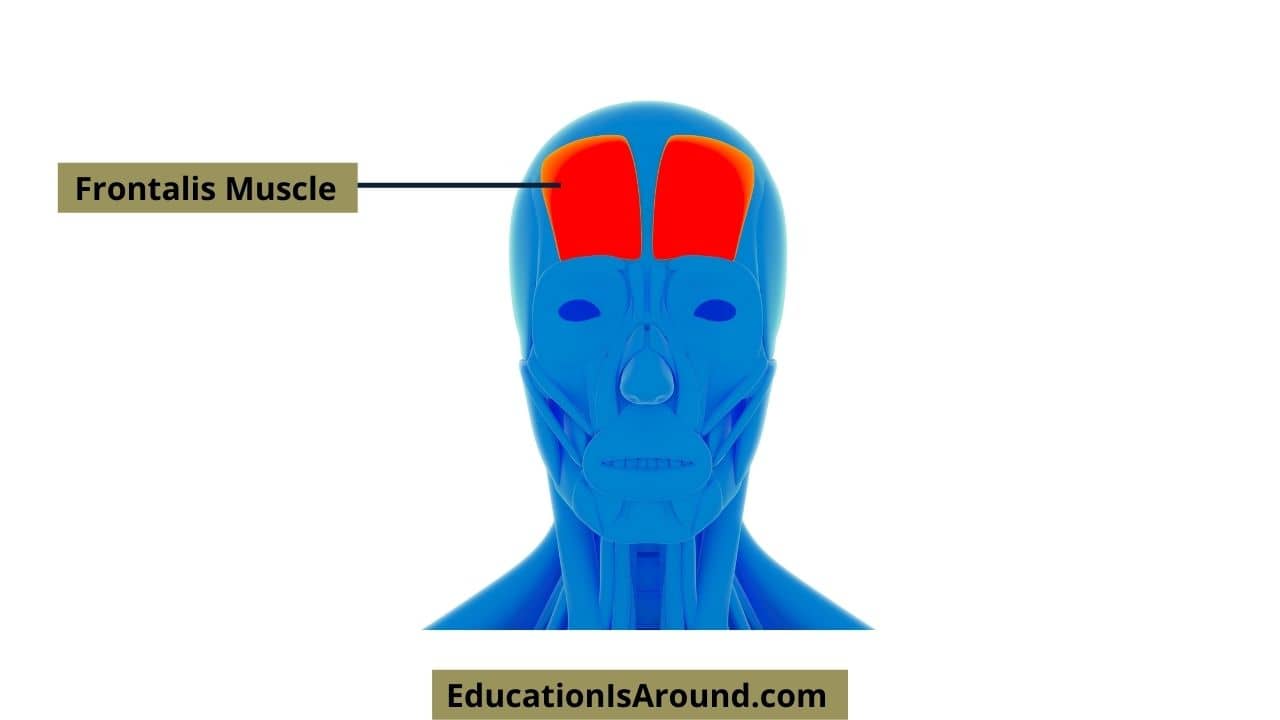
At the top of the skull (in the location of the forehead), the frontalis muscular tissue is a slim, vast, four-sided muscle mass. Mainly, this muscular tissue originates from the galea aponeurotica, expands down the temple, and inserts or affixes to the skin around the brows and the top of the nose. A sheet of fibrous cells covers the top of the skull called the galea aponeurotica.
The frontalis muscular tissue runs in the temple, in between the galea aponeurotica, the eyebrows, and the nose’s top.
Frontalis Muscular Tissue: Beginning & Insertion
Though the frontalis muscle mass may appear to be an independent muscular tissue, it is a part of a larger framework called the occipitofrontalis muscular tissue or epicranius. SCALP is a useful phrase for bearing in mind the layers of the scalp:
S: Skin
C: subcutaneous connective cells
A: Aponeurosis (galea).
L: Loosened areolar connective tissue.
P: Periosteum.
As opposed to one muscle mass tummy as the occipitofrontalis, it consists of 2 muscular tissue stomaches: the frontalis and occipitalis, which are linked and enclosed by a thick fascia called the epicranial aponeurosis or galea aponeurotica.
The occipital part of the occipitofrontalis muscle mass relocates the scalp onward, while the frontalis part raises the brows and relocates the former scalp backwards. The vertical fibres in the frontalis muscle pull the brows upwards when it contracts.
The superficial musculoaponeurotic system (SMAS) continues above the zygomatic arch and consists of the temporoparietal fascia (which mixes with the galea) and frontalis muscular tissue part of the SMAS.
The orbicularis oculi, corrugated, and procerus muscle mass work as antagonists to the frontalis muscle mass. There is no bony accessory to the frontalis muscle. The corrugator muscle mass lies listed below the frontalis and the orbicularis forces and has a bony beginning from the medial orbital rim.
Surface area Makeup
The frontalis muscle generates straight temple lines. The sorts of temple lines are as follows:
- Lines that run straight throughout the whole temple (45%).
- Gullwing forms with a central clinical depression and side altitude (30%).
- There are a few or no straight lines side the temple’s centre (10%).
- Lateral straight lines create two columns on the lateral aspect of the temple without any main lines (15%).
Frontalis Muscular Tissue: Muscle Structure.
The frontalis muscle is made up of vertical striations in a fan-like pattern. In some cases, muscular tissue is clinically split into median, intermediate, and side fibres despite no physiological or histological distinction. From the galea aponeurotica, which corresponds with the hairline on the surface, it emerges posteriorly.
On the inferolateral side, the muscular tissue interdigitates with the procerus muscular tissue fibres. On the inferomedial side, it has add-ons to the orbicularis oculi and corrugator muscle mass. Typically, the frontalis inserts at the brow dermis and terminates side to side at the temporal ridge. However, there are exemptions, and the frontalis might sometimes end even more medially.
Regardless of being a lean muscle mass with high vascularity, its bulk is located right over the brow. It is narrowest from side to side, which is a sign of a weak point and the initial location to sag with age.
When gauged from the supraorbital notch, the lateral level of the frontalis muscle, where it interdigitates with the orbital orbicularis muscle, maybe tiny, medium, or significant. The exact distribution in the common populace is unidentified.
When the straight frontalis is smaller, the lateral brow will undoubtedly have less assistance, bringing about eyebrow ptosis and lateral brow ptosis with the second dermatochalasis.
Few more details
At 20%, the lateral-most extent of the frontalis muscular tissue is crooked where it interdigitates with the orbital orbicularis muscle. Asymmetrical lateral eyebrow ptosis and secondary dermatochalasis might result from this arrangement. A research study has located similar variants in the length of the corrugator muscular tissue as being short or long. However, it revealed no distinctions in the procerus or orbicular muscular tissues.
According to a research study, the ideal stubborn belly of the frontalis muscular tissue is dramatically more significant than the left side. However, electromyographic research has shown the muscle mass on both sides is equally active.
It is feasible for the frontalis muscular tissue to be confluent from right to left with no bifurcation (as much as 45% of topics). There will undoubtedly be a variable main bifurcation in between the frontalis muscles in the remainder of the workouts. It consists of connective cells that bisect the galea aponeurotica, with varying widths from one person to another.
In 15% of anatomical breakdowns, Abramo et al. discovered the complete separation of the frontalis muscle mass tummies with a central galea aponeurosis.
A third of subjects have a gross asymmetry between the right and left frontalis muscular tissue stubborn belly.
There is evidence that the angle between where the frontalis interdigitates with the orbital orbicularis muscle mass may be tiny, medium, or significant. It may lessen with age, creating further lateral brow ptosis and additional dermatochalasis.
The lateral side of the frontalis muscle might reach the temporal crest, might expand past it, or may disappoint.
Frontalis Muscle Mass: Feature
As you did at the start of this lesson, the frontalis muscular tissue is responsible for raising the brows and wrinkling the forehead. As the frontalis muscle mass inserts or connects to the skin around the brows, as this muscle contracts, the skin around the eyebrows is pulled upwards, which raises the brows.
For the frontalis muscle mass to work, it must obtain electric impulses from the mind via cranial nerve VII, an innervation procedure. Cranial nerve VII is likewise referred to as the facial nerve.
Keep in mind the last time you were surprised or scared. Perhaps you watched a scary flick, or your loved ones stunned you on your birthday. How did your face look when you were frightened or surprised? Most people increase their brows and wrinkle their foreheads when they are surprised or anxious. Because of this, the frontalis muscle is used to develop these types of faces.
The frontalis muscle mass lifts the brows and creases the forehead, a usual expression of being shocked or frightened.
Embryology
In addition to the various other muscular tissues associated with facial expression, the frontalis stems from the second pharyngeal arch, which develops between the 3rd and 8th weeks of development.
The Blood Supply and also Lymphatic System
The internal and exterior carotid arteries supply blood to the frontalis muscle mass. Upon exiting the orbit and taking a trip up the forehead, the supratrochlear and supraorbital arteries provide the muscular tissue from the substandard margin. The supraorbital artery can leave with the supraorbital notch/foramen, while the supratrochlear artery exits much more medially from the orbit.
They are both branches of the internal carotid artery, a branch of the ophthalmic artery. Following their particular leaves, the supratrochlear and supraorbital arteries divided better right into superficial and deep branches.
The superficial vessels supply muscular tissue, galea, and skin, while the deeper vessels supply the periosteum. The supratrochlear and supraorbital arteries provide a lot of the blood medially, while the frontal branch, which comes from the superficial temporal artery, supplies the blood from side to side. Throat arteries create an anastomosis with each other to create a highly vascularized network.
The lymphatic water drainage of the temple is intricate and poorly recognized. According to studies on the drainage of the forehead, the lateral portions drain differently than the medial sections. Regardless, the forehead drains pipes mainly right into the preauricular nodes and parotid nodes.
Critical venous drainage occurs between three capillaries: the supratrochlear capillary is one of the most medial, adhered to by the intermediate supraorbital blood vessel, and finally, the side frontal blood vessel. A transverse vein that runs above the orbit better attaches the three, adequately called the transverse supraorbital blood vessel.
The transverse supraorbital vein attaches medially to the angular blood vessel, which drains right into the spacious sinus and ocular blood vessel. Relating to the threat of exterior facial infections causing possibly harmful intracranial infections or cavernous sinus apoplexy, it is essential to keep in mind this connection.
Nerves
The muscular tissues of the face are supplied with nerve fibres by the cranial nerve VII (the facial nerve), which includes five major branches: temporal, zygomatic, buccal, minimal mandibular, and cervical. At the stylomastoid foramen in the head, the facial nerve arises, as well as the earthly branch of it crosses over the zygomatic arch, passing through the areolar tissue that makes up the surface of the temporal fascia and consequently becomes part of the frontalis muscular tissue to offer deep innervation to the muscle mass.
The temporal nerve has three branches, the former, centre, and posterior, which innervate the orbicularis oculi, frontalis, and corrugator muscles. Also, temporal (or frontal) branch of the facial nerve exists within the surface layer of the temporoparietal fascia together with the temporal artery that runs just anterior to the nerve.
The temporal branch gets in the deeper part of the frontalis muscle from the material component. By cutting subcutaneously or simply anterior to the surface part of the deep temporal fascia (the glowing layer just in front of the temporalis muscular tissue), it is possible to prevent injuring the earthly branch of the facial nerve.
Two supratrochlear and supraorbital nerves leave the same arteries and penetrate through the frontalis to the superficial skin. They are branches of the ophthalmic department of the trigeminal nerve and do not directly innervate the muscle mass but instead innervate a layer of skin overlying the muscle mass. As the name implies, the median branches of the supraorbital nerve are shallow, and the side branches are deep.
Frontalis Muscular Tissue: Surgical Considerations
Understanding the composition of the frontalis is essential for rebuilding and cosmetic treatments. Suppose a kid is born with an absent or useless levator palpebrae superioris, as in reciprocal hereditary ptosis. In that case, the ptosis might be so severe that it triggers vision blockage and amblyopia.
Frontalis-orbicularis muscle development is possible in those clients. First described more than 100 years back, the procedure includes cutting the crease of the top eyelid, complied with by upright stakes right into the frontalis muscle.
Lastly, the muscle flap is progressed inferiorly to get in touch with the orbicularis oculi muscular tissue. Ptosis modification using the frontalis is also called frontalis slings or frontalis suspensions. This procedure is frequently favoured to muscle mass flap innovations and involves a similar approach, other than it utilizes a stitch to attach the frontalis to the tarsal plate.
This gives the needed pull to elevate the eyelid with frontalis contraction, comparable to the flap. Ptosis can result from mechanical, neurological, stressful, or muscle dysfunctions, every one of which can be treated by surgical procedure.
Frontalis Muscle Mass: Professional Importance
Improved temple skin:
To maintain a youthful look, people commonly look to invigorate the forehead. As we age, kicked back skin tension lines, likewise known as wrinkles, show up vertical to the underlying muscles. To decrease lines, vascular adjustments, and skin pigment modifications, nonsurgical treatments are commonly the primary step. There are nonsurgical choices such as creams, peels off, abrasives, and lasers.
Use botulinum toxic substance for the temple as well as frown lines:
In minimally invasive treatments like botulinum shots, anatomy plays an important role. Botulinum toxin works for treating rhytides and creases and injected directly into the frontalis muscle mass. The reduced muscular contraction leads to a decline in rhytid manufacturing and an extra younger look.
Several shots into the frontalis associate with this procedure. It is necessary to clarify complete paralysis of the frontalis muscular tissue: 10 to 20 units of botox distributed across the forehead creates satisfying leisure for the straight rhytids. Along with the frontalis, the corrugator and procerus muscles must also injected.
Two centimetres over the eyebrow is the secure zone for injections into the frontalis muscle mass. Improperly experiencing the contaminant can cause nonpermanent ptosis of the levator palpebrae superioris. Maintaining equilibrium between the levators and also depressors of the eyebrow is also crucial.
The brow will come down when the frontalis muscle is weak, and the depressors lead. Furthermore, improper circulation of botulinum into the median frontalis can create a “Spock” deformity. The side portion of the frontalis can cause contraction while the median part is unwind.
One location of frontalis activity that typically goes unattended, especially in females, is where the frontalis closes to the former hairline, where noticeable residual high straight rhytids result.
Fillers for grooves at the glabella:
Commonly, fillers are place into the temple to boost the volume and fullness of the horizontal lines at the root of the nose (triggered by the procerus muscle). The verticle “elevenses” at the median end of each brow are cause by the corrugator muscle mass.
A thorough understanding of the underlying composition, including the depth and area of the various muscles, is vital for avoiding damaging issues. Too much filler or a misplaced filler in the glabella (the location between the brows and over the nose) can block the retinal arteries and trigger loss of sight. A wrong shot into an artery might create a loss of sight.
Supratrochlear, for example, might cause acute death of the cells. Injections of fillers are never compel or boluse. On top of that, we have located that infusing small amounts of filler delicately right into the skin upwards is a safe method of dealing with creases.
Upper and also reduced motor nerve cell face palsy:
When examining an individual with a stroke, it is likewise critical to recognize the nerve supply to the forehead. Strokes of the middle cerebral artery can cause contralateral facial paralysis. Yet, these strokes hardly ever affect the temple because the lower electric motor nerve cells responsible for innervating the top half of the face receive input from both hemispheres but not the reduced half. In the case of Bell palsy, we see complete hemifacial paralysis when the lower motor neuron wound.
Tissue development:
When fixing big temple or nasal issues, cell development needs. In the neck, the expanders place in front of the platysma. However, it is crucial to put the expanders underneath the frontalis muscle mass in the temple, with incisions made in the hairline.
Other Problems
- The frontalis muscle is part of the occipitofrontalis muscle, which is two stubborn muscle bellies connect with the galea aponeurotic.
- Cavernous sinuses get part of the venous drainage from the temple.
- The frontalis muscular tissue elevates the brows, whereas the corrugator supercilii, orbicularis oculi, and procerus play a role in its anxiety.
- In centre cerebral artery strokes, the feature of the forehead is frequently spare.
- To avoid injury to the sensory and motor nerves of the frontalis muscle, dissection aeroplanes need to be subcutaneous, subperiosteal, or subgaleal.
- The medial branches of the supraorbital nerve are superficial, while the side branches are deep.
- Variations in the straight level of the frontalis muscle must thought about, as these variants might influence the level of eyebrow ptosis.
- An appreciation of the surface and applied composition of the temple and the level of the frontalis muscle need when performing surgery in this area or injecting toxic substances into it.
FAQs
What is the feature of the frontalis muscular tissue?
The frontalis muscular tissue boosts the brows, while the corrugator supercilii, orbicularis oculi, and procerus play a role in its clinical depression. The temple is usually save when a stroke happens between the cerebral artery.
Where is the frontalis muscle mass, and what does it do?
The frontalis muscles are the temple’s up and down oriented muscles that raise the brows. One increases the eyebrows by acquiring the forehead muscle and simultaneously develops straight forehead creases.
How do I relax my frontalis muscle mass?
Relax your frontalis muscular tissue by resting easily and lowering your brows as high as possible while frowning. Hold this setting for 5 seconds, then elevate your brows as high as possible while smiling. Hold this position for five seconds. After that, repeat the entire exercise ten times.
Frontalis connects to?
Considering that the frontalis muscular tissue connects to the skin around the eyebrows, its primary function is to increase the brows, triggering the skin of the temple to crease.
What kinds of faces are enable by the frontalis muscular tissue?
Frontalis muscle mass– raises the brows, makes straight temple creases when we appear surprise. Orbicularis oculi– the round muscle mass of the eye (contains two muscular tissues). It shuts the eyelids and squints the eye.